DREZ LESIONING
What we do?
We provide advanced surgical and non-surgical treatments for Brachial Plexus Injuries and chronic neuropathic pain using cutting-edge neuromodulation and microsurgical techniques for long-term relief.
Brachial Plexus Care
Expert management of traumatic, birth-related, and tumor-associated brachial plexus injuries to restore arm movement, strength, and sensation.

Pain Management Expertise
Comprehensive solutions for severe neuropathic pain through medication, nerve blocks, and neurostimulation therapies tailored to each patient’s condition.


DREZ Surgery
Specialized in performing DREZ lesioning for patients with avulsion injuries, offering up to 80% pain relief by targeting the damaged pain pathways in the spinal cord.

Advanced Diagnostic Approach
Accurate evaluation using MRI, neurophysiology, and imaging to determine the extent of nerve damage and identify the best possible treatment plan.
DORSAL ROOT ENTRY ZONE (DREZ)
Brachial Plexus Injuries are caused by excessive stretching, tearing, or trauma to a network of nerves from the spinal cord to the shoulder, arm, and hand. Injuries often occur secondary to motor vehicle accidents, sports injuries or surgeries. Traumatic BPI causes either complete or incomplete damage to the brachial plexus resulting in loss of function and sensation related to level of damage. The recovery from the injury will depend on the severity, level and type of nerve damage. Pain is a very important side effect of the injury and can sometime be very severe and debilitating.
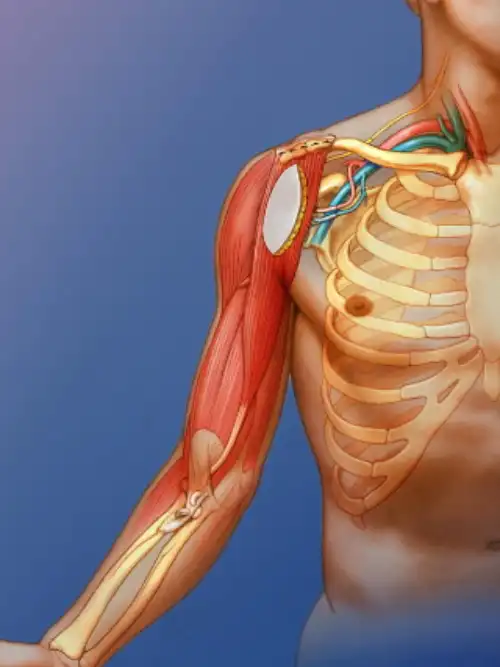
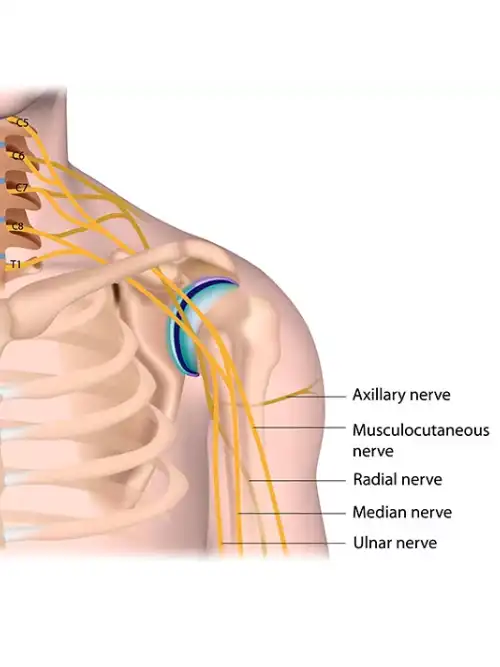
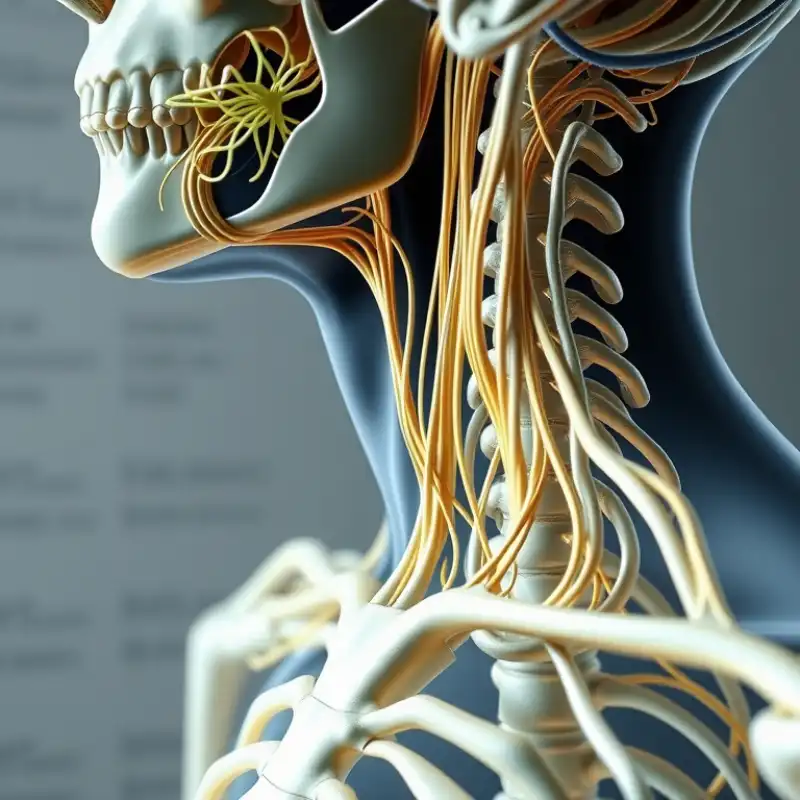
What is the brachial plexus?
The brachial plexus is a network of nerves in the neck and shoulder region (see the video above). It is made up from 5 large nerves which come out of the spinal cord between the vertebrae (bones in the neck), pass under the clavicle (collar bone) and into the upper arm. These nerves enable the signals that allow movement and feeling to reach the arm. These nerves are represented in speech and writing by these symbols: C5, C6, C7, C8, T1 (C=cervical, T=thoracic)
What are nerves and the nervous system?
Nerves are cord-like structures made of numerous nerve fibers that transmit electrical signals between the brain, spinal cord, and body tissues. They enable movement and sensation by carrying messages from the brain to muscles and sensory information back to the brain. When nerve fibers are damaged, the connected muscles may weaken even if the muscle itself is unharmed. The nervous system functions by sensing changes, interpreting them, and triggering appropriate motor responses through sensory and motor neurons.
What are the causes of BPI?
Damage to the upper nerves that make up the brachial plexus tends to occur when your shoulder is forced down while your neck stretches up and away from the injured shoulder. The lower nerves are more likely to be injured when your arm is forced above your head. These injuries can occur in several ways, including:
1. Contact sports
During football, players can experience stretching to the brachial plexus beyond their limit during collisions with other players.
2. Trauma
Traumatic brachial plexus injuries may arise from several causes, including sports, high-velocity motor vehicle accidents, especially in motorcyclists, falls from a height, direct violence or gunshot wounds and other accidents
3 Tumor
Noncancerous (benign) or cancerous tumors can grow in the brachial plexus or put pressure on the brachial plexus or spread to the nerves, causing damage to the brachial plexus.
4. Difficult births
Newborns may suffer brachial plexus injuries during difficult births, causing nerve damage like Erb’s palsy or total plexus palsy.
5. Radiation treatment
Radiation treatment may cause damage to the brachial plexus.

What happens when there is an injury of the brachial plexus?
Symptoms of Brachial Plexus Injury may include
- Paralyzed of whole upper limb or part of it - loss of muscle control in the shoulder, arm, hand, or wrist,
- Lack of feeling or sensation in the arm or hand.
- Pain along the distribution of the nerve complete or in complete.
1. The number of nerves affected
This varies between patients. Sometimes only one or two nerves are damaged resulting in loss of movement in one area, e.g. shoulder or elbow. In some cases, all the nerves are damaged causing complete loss of movement and feeling in the arm.
2. How badly the nerves have been damaged
There may be mild stretching or compression of nerves. However, in more severe injuries, nerves may be torn apart by severe stretching. Deep wounds may cut through the nerves.
How do I know how severe the brachial plexus injury is?
We may be able to determine the degree of damage to the nerves by examining you. However, it is quite common for other tests to be done to help tell us where the nerve injury is and how bad it is. These tests may include:
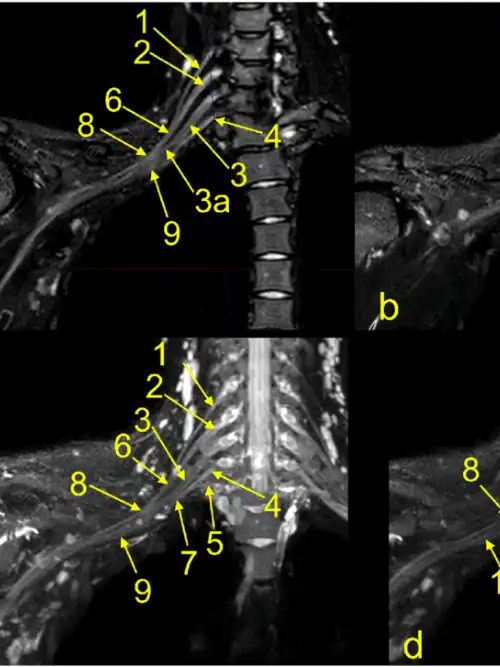
1. MRI scan
This will provide information about the number of nerves damaged, spinal cord injury and formation of a swelling in the covering of the spinal cord.
2. Neurophysiology
Recording of the passage of electrical signals along nerves in the limbs using small electrical pulses on your skin. The test may include a recording of the electrical activity of muscles which involve using fine needles. These tests can be used to diagnose a variety of nerve or muscle problems.
Can BPI happen during birth?
Many brachial plexus injuries happen during birth, if the baby’s shoulders become impacted during the birth process, causing the brachial plexus nerves to stretch or tear. Some brachial plexus injuries may heal with little or no treatment. Many children improve or recover by 3-4 months of age. To expand range of motion and speed rehabilitation, physical and occupational therapies are usually employed.

What symptoms do patients have with BPI
A brachial plexus injury can be life changing and you may experience some differences in the following areas of your life:
1. General health
Insomnia (sleeplessness), fatigue, loss of appetite, weight loss or gain (this may be related to your medications). These symptoms usually resolve over time.
2. Daily living
Difficulty in carrying out everyday activities including your current work, future employment concerns, participation in sports and hobbies, doing housework and child care, shopping etc
3. Psychosocial
You may experience poor focus, low confidence, anxiety, frustration, and emotional distress similar to grief, often accompanied by guilt, irritability, and loss of interest in daily activities.
Psychosocial effects in patients with BPI may include

Anxiety
Anger

Denial

Depression

Acceptance
How does BPI affect someone’s life?
Pain is a sensory and emotional experience which can cause serious psychological changes in the person. Pain develops early in 90% of brachial plexus injury cases, and it may be also delayed for 3-4 months. Generally the pain improves by 2-3 years and is usually manageable by the patients. But in 30-40% of patients the pain becomes very severe and unbearable. Pain after injury can be divided into paroxysmal (shock like) pain and continuous (burning) pain. The continuous pain is a chronic burning or stabbing pain that does not ordinarily follow a clear distribution and usually located in the forearm and the hand. The other paroxysmal pain is a sharp electric shock like pain which is crushing, very severe, lasts few minutes and can occur every few minutes and sometimes ‘like putting your hand in a deep frying pan’. Some of the characters of the pain described by the patients are as follows, “ my arm is on fire with continuous electric shocks 24 hours, even a small noise like tapping aggravates pain, I wanted to end my life and attempted suicide several times, I used to have 24hrs pain very slightly reduced with tablets, pain will start from hand all the way up to neck, pain was like pin pricks or someone was stabbing my arm and every time it was different, 22yrs I had pain and even the slightest noise like a baby crying will set it off, I chewed my hand daily for pain relief as it was like on “burning oil”.

An Accident Can Never Claim Your Happiness
It is time to bid good-bye to the severe neuropathic pains! Dr G. Balamurali, with his extensive experience in the field and 80% success rate is here to help you get rid of the pain!
What are the treatment methods that Dr G Balamurali can offer for pain?
The treatment methods for pain relief are surgical methods or non-surgical methods. We will discuss about both methods in detail below.
Non-Surgical Methods
Some of the medications used to treat pain are
Medical management can fail after sometime when either a single drug or combinations of drugs have been taken up to the maximum acceptable dose for a duration of few months to years or when side effects do not allow you to take the medication that is required. When such a situation arises it is wise to consider surgical options.
Surgery should be considered only when medical and other treatment methods have failed over a period of 6 months to 2 years and the patient can no longer accept the pain.
- Non steroidal anti inflammatory (NSAID’s)
- Tramadol
- Anti epileptics e.g. gabapentin, pregabalin, carbamazepine, lamotrigine, Gabapentin
- Anti depressants e.g. amitryptyline, duloxetine
- Topical medicines – E.g. gels, creams, patches
- TENS (Transcutaneous Electrical Nerve Stimulation)
Surgical Methods
In BPI the nerve can be pulled our or disconnected from the spinal cord. The region where it gets disconnected undergoes scar tissue transformation and become a focus of pain generation. This region is called the “Dorsal Root Entry Zone” (DREZ), which is the first important level of modulation for pain and hence this area can be a target to treat resistant neuropathic pain in avulsion injuries.
- Nerve block surgeries
- Intrathecal pumps delivering painkillers direct to the area affected
- Ablative (destructive) surgeries, which involve the burning of nerve endings - DREZ
DREZ Operations
The dorsal root entry zone (DREZ) lesioning procedure is a treatment for severe pain caused by nerves that have been torn away (avulsed) from the spinal cord. The procedure itself involves a neurosurgeon entering the spinal cord and causing multiple lesions in that damaged areas of pain generation from the spinal cord. Dr G Balamurali is among the very few Surgeons in the Country who has vast experience in performing this procedure under neuromonitoring. We have a 80% success rate.
Please visit our support group www.bpisupportgroup.com
Drez Lesioning Videos
Patient Testimonial - DREZ Surgery in Leg
Kiran Testimonial
Dorsal Root Entry Zone (DREZ), Brachial Plexus Injury
Brachial Plexus Injury - Dr G Balamurali, Spine and Neurosurgeon, Kauvery Hospital, Chennai, India
Brachial Plexus Injury - DREZ surgery - Dr G Balamurali - Spine and Neurosurgeon, Kauvery Hospital
Brachial Plexus Injury - www.bpisupportgroup.com - Dr G Balamurali talk
Brachial Plexus Injury - Dr G Balamurali, Spine and Neurosurgeon, Kauvery Hospital, Chennai
Brachial Plexus Injury - www.bpisupportgroup.com - Dr G Balamurali talk
Dorsal Root Entry Zone (DREZ), Brachial Plexus Injury
Dorsal Root Entry Zone Surgery, outcomes after Brachial Plexus Injury surgery
Dorsal Root Entry Zone, DREZ , Brachial Plexus Injury Surgery
Patient Testimonial for Dr G Balamurali
Patient Testimonial following Surgery with Dr G Balamurali
DREZ surgery technique, Dr G Balamurali, Spine and Neurosurgeon, Kauvery Hospital, Chennai, India
In Association With

